
- What is Vesicoureteral Reflux (VUR)?
- What causes VUR?
- What are the symptoms of VUR?
- How is VUR diagnosed?
- How is VUR treated?
What is Vesicoureteral Reflux (VUR)?
VUR is the retrograde flow of urine from the bladder to the ureter, usually during the effort of micturition. Normally, at the vesicoureteral junction (meeting point of the ureter with the bladder), there is a valvular mechanism inhibiting urine reflux. When this mechanism is either absent or insufficient in some children, VUR occurs. VUR incidence rate in children is about 1%. In kids with renal pelvis dilatation, the disease has an incidence of about 16,2%. Kids whose parents used to have VUR during their childhood, develop VUR in 35,7%. Also, it is more common in children with urinary tract infections (30-50%). Therefore, every child with urinatry tract infection should be tested for the disease. Though rare in adults, VUR may occur in grown-ups who have history of benign prostate hypertrophy, neurogenic bladder or have undergone surgery in the region near ureter orifices.
What causes VUR?
Causes can be either congenital or acquired.
Congenital causes:
- Disruption of bladder trigone/ Primary VUR
- Double ureter
- Ectopic ureter
- Ureterocele
Acquired causes:
- Chronic urinary retention (when amounts of urine remain in the bladder for they cannot be discharged with micturition). This occurs in males above 50 y.o. due to prostate hyperplasia, as well as in patients with neurogenic bladder.
- Surgical operations in bladder neck, vesicoureteral orifices or for prostate hyperplasia.
What are the symptoms of VUR?
There are usually no symptoms in VUR. However, it may manifest symptoms similar to those of urinary tract infection with urinary frequency, fever and shivering. As long as there is retrograde flow of urine towards the kidney, there is inflammation induced in the kidney and pelvis, which is called pyelonephritis. Recurrent infections cause renal impairment and in some neglected cases may even destroy kidneys, resulting in renal failure. Renal impairment may be involved in the etiology of children's hypertension.
How is VUR diagnosed?
Today, with the wide use of ultrasounds during gestation, the suspicion for VUR is set already from fetal life. In other children, it is raised after investigating the urinary tract on the occasion of some urinary tract infection (UTI) .Tests recommended initially by the physician aim at evaluating the child's overall health condition and growth, UTI presence, renal function and severity of the disease. VUR screening includes:
- Clinical examination and history taking
- General urine test (urinalysis) and culture
- Blood test, for evaluating renal function
- Urinary tract Ultrasound (U/S), for evaluating any potential renal pelvic dilatation
- Urodynamic testing, for evaluating bladder function and micturition. The results will determine the therapeutic approach to a great extent.
- Cystourethrography. A specific radiological examination that is the method of choice providing the most detailed and accurate information about the disease and degree of severity.
- Alternatively, in order to avoid radiation, Cystourethrography can be conducted with radioisotopes in a nuclear medicine laboratory. However, this provides less information compared to classical cystourethrography and is usually used only in children's screening,
- MRI has been used during the last years, but there is need for further studies to provide more evidence supporting MRI value.
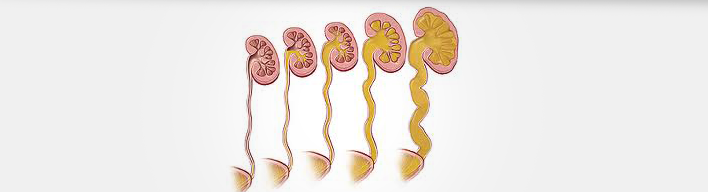
According to diagnostic screening, VUR is classified into five (5) grades (see picture above text). Grades 1 to 3 are more mild-moderate VUR cases, while grades 4 and 5 are the most severe ones. This classification is highly significant for the therapeutic plan to be decided.
How is VUR treated?
VUR in adults is usually treated surgically and aims at resolving the disease that causes it. Patients with neurogenic bladder, though, are an exception and are treated in specialized centres (see: Neurogenic Bladder).
In children, it is only in rare cases that VUR is treated surgically. According to studies, in the majority of children the problem is due not only to retrograde urine flow but also due to bladder dysfunction. Thus, the surgical procedure is conducted at the level of bladder function and is determined with urodynamic testing. Only in rare cases when the child keeps having UTIs despite chemoprophylaxis, surgical treatment is indicated.
- Irrespective of the reflux degree or presence of renal scarring, all children diagnosed with VUR within the first year of their life should be treated with chemoprophylaxis, that is continuous oral antibiotic administration for a long time, i.e. for six months or one year. In children suffering from feverish infections, there is need for intravenous therapy. However, kids who manifest frequent recurrent UTIs are strongly indicated for open or endoscopic surgery. Open surgical procedures seem to be more effective in children with high-degree reflux. In small degree reflux, endoscopic techniques (injection of special substances below the ureteral orifice for blocking the retrograde urine flow) have equally good results as open surgery.
- For children 1-5 years old, it seems that chemoprophylaxis is the treatment of choice for preventing kidney scarring. However, if reflux is severe, surgical treatment is an alternative solution. For mild reflux cases, endoscopic treatment is recommended if parents seek a definite resolution to their child's problem without the need of continuous follow-up and antibiotics.
- All children should be educated how to urinate properly.