
- What is Ureteroplevic Junction Stenosis (UPJ Stenosis)?
- How is UPJ Stenosis diagnosed?
- How and when is UPJ Stenosis treated?
What is Ureteropelvic Junction Stenosis (UPJ Stenosis)?
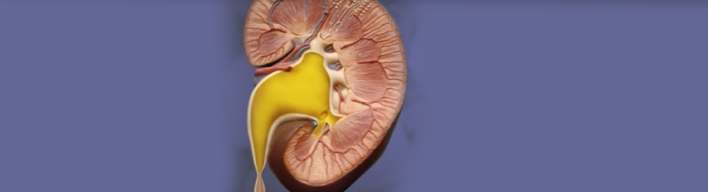
It is one of the most common benign diseases causing renal pelvis dilatation. It mosttly occurs in children and is mainly congenital (from birth). Ureteropelvic junction (UPJ) is the point where the ureter meets the renal pelvis. Renal pelvis is like a 'sink' collecting urine produced by the kidney, while UPJ is the 'sink-trap' (siphon) through which the urine has to pass so that it will end to the bladder through the ureter. Exactly at that point there is a stenosis obstructing normal urine flow; as a result, the urine pools in the renal pelvis, compresses it and ultimatly induces its dilatation. It occurs in approximately 1:1500 children, while the ratio boys/girls is 2:1.
How is UPJ Stenosis diagnosed?
Prenatal UltraSonography
Today, the wide use of ultrasound (U/S) during gestation raises the suspicion for UPJ obstruction even from fetal life. The first indications are usually demonstrated in the ultrasonographic screening conducted during the 16th-18th week of gestation. Yet, the degree of stenosis is evaluated during the 28th week of gestation.
U/S after birth
After birth, there follows ultrasound screening. Given that the newborn is dehydrated during the first 24 hours, the test should be conducted 48 hours after birth so that the results are reliable.
Voiding Cystourethrography
It is a special radiographic examination, aiming at excluding other congenital diseases causing renal pelvis dilatation. These diseases are diagnosed up to 25% in children with renal dilatation. Such conditions are Vesicoureteral Reflux (VUR), Neurogenic Bladder, Ureterocele and Posterior Urethral Valves.
Dynamic Renal Scintigraphy
This examination provides information about the obstruction and how this may potentially affect renal function. It has to be conducted between the 4th and 6th week of gestation.
How and when is UPJ Stenosis treated?
Before birth
If the problem is severe and there is high risk for affecting fetal growth, there may be need for some intervention during intrauterine life. This is extremely rare and has to be performed only in highly specialized centres with great experience.
After birth
When dilatation is small, renal function has not been affected and there are no symptoms (pain, urinary tract infections), the child should just be monitored on a regular basis. In other cases, though, the stenosis has to be treated. It is important to reassure parents that renal dilatation is not always correlated with renal impairment and that the treatment has specific indications. There is greater experience and longer follow-up in open surgical interventions. Yet, more and more centres present data from laparoscopic and robotic surgical methods for the restoration of the problem. Results seem to be equally good but longer follow-up of patients is needed to provide sufficient evidence.