
- What is Erectile Dysfunction (ED)?
- Is ED still a taboo-subject?
- What is known today about ED?
- How common is ED?
- In which age group is ED more common?
- Does the problem occur also in young men?
- What are the most common ED causes in young men?
- What are the most common ED psychogenic causes?
- What is the effect of wrong attitude towards ED?
- Until what age should a man with ED ask for help?
- What are the most common ED causes?
- How is ED diagnosed?
- Which are the ED diagnostic tests?
- Is there a test discriminating between psychogenic and organic ED?
- How is Vascular Erectile Dysfunction (VED) diagnosed?
- What therapeutic options are available today?
- What are the most widely applied therapies today?
- How effective and safe are Erection Pills?
- Are there differences among ED oral drugs?
- How many Greek men take ED oral drugs today?
- If erection pills are not effective, what other therapeutic options are available?
- Besides pharmacotherapy, what other therapeutic options are available?
- What is the new Erectile Dysfunction Shock-Wave Therapy (EDSWT)?
- What are Shock-Waves (SW)?
- How is EDSWT applied and how effective is it?
- How effective are drugs that are advertised on T.V/ mass media and are purchased from drug stores without medical prescription? Should we trust them?
- How safe are drugs ordered online (on the Internet??
- Do also men without ED take erection drugs?
- What can I do for prevention?
What is Erectile Dysfunction (ED)?
The continuous or intermittent inability to achieve or maintain erection for satisfactory sexual intercourse. This term is different from the term of sexual dysfunction which is broader including disorders of sexual desire, ejaculation, orgasm and satisfaction. A transitional ED episode is not necessarily important and can occur to anyone. If this, however, is repeated or becomes permanent, you should promptly consult your physician. If you do not treat it, it may probably cause discomfort, stress and problems to your relationship and reduce your self-confidence. No matter how uncomfortable you may find it to talk about something so personal to your doctor, you should be aware that ED is a health problem that can certainly be treated.
Is ED still a taboo-subject?
Although many men experience this unpleasant condition for a long time, the vast majority do not resort to an expert physician for resolving the problem. This hesitation to seek help is characteristic not only in Greek men. Different international studies have recorded embarrasment as the main reason. It was also found that young men find it even more difficult to address themselves to the physician compared to men of more advanced age. This is related to the myth and misconception that sexual problems arise only at older ages. The first step is always hard to be made, but it surely is the only 'key' for resolving the problem.
What is known today about Erectile Dysfunction?
During the last 25 years, the mechanism of erectile dysfunction has become clear. We have learnt the etiology and incidence rate, and have invented diagnostic tests ot identify the problem. As from treatment, we have moved from invasive therapies -with penile prostheses and intrapenile injection in the decade of the 80s- to the breakthrough of oral drugs -with the introduction of sildenafil (Viagra ™) in 1998. Then followed tadalafil (Cialis™) and vardenafil (Levitra™). Recently another great stride has been made with Shock Waves, a therapeutic method not only treating the symptom but also aiming at the cause of the problem when this is of vascular origin. There is no other medical field that has developed so rapidly within such a relatively short period.
How common is ED?
The incidence rate of ED increases as age advances. Thus, at the age below 40 y.o. the problem occurs in 1 out of 20 men; in the age group 40-60 y.o. , it occurs in 1 out of 10 men; and above 60 y.o. it occurs in 1 out of 5 men. In Greece, it is estimated that there are more than 500.000 men living with the problem.
In which age group is ED more common?
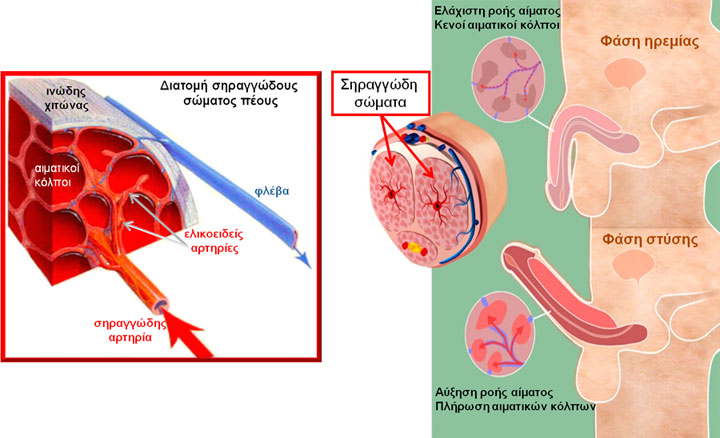
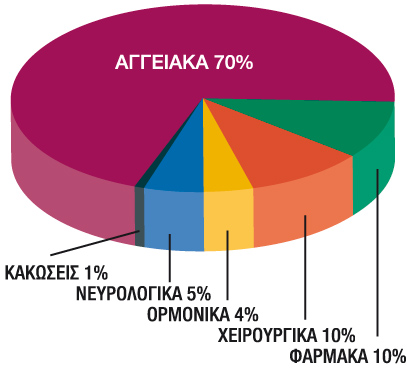 After the age of 50, men usually have an organic problem. Erection is a vascular phenomenon, since blood flow is absolutely crucial for achieving erection; blood flow has to increase so that the penis fills with blood. This explains why 70% of erectile problems of organic etiology are due to vascular origin. A bad-quality erection may even indicate a heart problem. Studies have demonstrated that vascular erectile dysfunction usually precedes the onset of coronary disease by 3 years. Your Urologist, can identify whether there is vascular etiology, with the application of a novel imaging test, the Triplex Ultrasound of penile vasculature.
After the age of 50, men usually have an organic problem. Erection is a vascular phenomenon, since blood flow is absolutely crucial for achieving erection; blood flow has to increase so that the penis fills with blood. This explains why 70% of erectile problems of organic etiology are due to vascular origin. A bad-quality erection may even indicate a heart problem. Studies have demonstrated that vascular erectile dysfunction usually precedes the onset of coronary disease by 3 years. Your Urologist, can identify whether there is vascular etiology, with the application of a novel imaging test, the Triplex Ultrasound of penile vasculature.
Does the problem also occur in young men?
Organic causes are more rare at ages below 50 y.o. However, satisfactory sexual performance presupposes not only good organic function of the body but also proper activation of psychological mechanisms. All studies demonstrate that 9 out of 10 healthy men below the age of 40, experience some sexual problem that is of psychogenic etiology. Many men find it hard to accept that their problem might be psychological. This reflects the common male belief and misconception that psychological problems are a sign of weakness and a man has must always be able to overcome these problems on his own without asking for help. In most cases, however, when an erectile problem emerges, this is due to a randomly occurring 'bad instance' when the man once happened to fail in achieving or maintaining his erection.
What are the most common ED causes in young men?
In young men, the problem usually occurs at the onset of their sexual life or in a new relationship or even due to the use of condom. An occasional failure, at some point in their life, may probably make them feel anxiety for the next time and a second failure will lead to a series of unsuccessful attempts. Under such a psychological stress, the man can no way focus on and respond to sexual stimuli; thus,erection may not be achieved or, if achieved, is lost during sexual intercourse (most times after penile penetration). He perceives this as as a significant failure making him seriously worry about whether he will be able to respond next time, and this leads to a repetition of the negative experience. As a consequence, the man becomes obsessed with and focuses only on the quality of his erection instead of trying to please his sexual partner by sending and receiving sexual stimuli. This condition is called 'Sexual Performance Anxiety' and is very often the only cause of the problem. This anxiety increases with every experience of unsuccusful erection, resulting in a vicious circle that many times may lead even to avoidance of sexual intercourse.
What are the most common ED psychogenic causes?
|
ED etiology may very often include:
|
|
|
|
|
|
|
|
|
What is the effect of wrong attitude towards ED?
Studies in different social and cultural populations have demonstrated that erectile problems are more common in men who believe that they must always have erection irrespective of circumstances and that they must always be able to satisfy their sexual partner's sexual needs. Such convictions and misconceptions are deeply rooted even inside the most consistent and mature men. However, it seems that they favor the development and maintenance of performance anxiety!
The key to the problem is for young people to seek help from a Trained Sexologist, who will help them overcome the problem soon. Yet, instead of addressing themselves to Trained Psychologists/ Psychiatrists, they prefer either to remain silent or resort to the 'easy solution', that is erection drugs. However, they have to fully realize and accept that ED is a medical problem and they should not hide it! The longer the therapy is delayed, the harder the problem gets to treat!
Until what age should a man with ED ask for help?
Sexual activity reduces with age. Even though scientific data demonstrate that sexual life plays a very important role in the life quality of people of all ages, many people doubt its significance at the third age. The truth is that, as long as a man has sexual desire, age is not a deterrent factor. Therapies that are available today are safe even for older ages and should be provided to everyone, as long as there are no contra-indications.
What are the most common ED causes?
Erection is an exceptionally complex procedure involving brain, hormones, nerves, muscles, vessels and, of course, emotions and higher mental functions, such as senses, memory and attention. Any disorder along this procedure may become a cause of erectile dysfunction. Even though problems may be of organic origin, anxiety and stress will certainly arise and aggravate the problem; or even the opposite may occur. Very often there may be a combination of both organic and psychological factors from the very beginning.
The most common organic causes are:
- Heart diseases
- Vascular occlusion
- High levels of cholesterol and triglycerides
- High blood pressure
- Diabetes mellitus
- Metabolic syndrome (combination of excess body fat around the waist, high blood pressure, high insulin levels, high cholesterol)
- Obesity
- Neurological diseases (e.g. bone marrow injuries, Parkinson's disease, multipls sclerosis)
- Hormonal disorders (e.g. low testosterone)
- Peyronie's disease ( (formation of scar tissue known as 'plaques' within the tunica albuginea of the penis)
- Pharmaceutical agents (antipsychotics, antidepressants, antihistamines, diuretics, antihypertensives etc)
- Smoking
- Drug abuse
- Alcoholism
- Therapies for prostate cancer ( hormonal therapies, radiotherapy, radical prostatectomy)
- Prostate hyperplasia (often concomitant with erectile dysfunction)
- Pelvic surgery (e.g. of the colon, bladder or prostate)
The most common psychological causes are:
- Myths and misconceptions related to sex and sexual performance
- Anxiety/ Stress
- Low self-esteem
- Problems in family or relationship
- Difficulty in conceiving (unsuccessful attempths for successful pregnancy) - Infertility
- Sexual performance anxiety/ Attention deficit disorder
- Anxiety disorders
- Poor sexual communication with sexual partner
- Depression
- Psychiatric diseases (e.g. schizophrenia, personality disorders etc)
How is ED diagnosed?
The Urologist will initially take your detailed medical and sexual history. You should speak honestly and always remember that your physician is trained to talk about such sensitive and personal issues. So, do not hesitate to speak openly so that he can really help you.
During the first visit, the physician wants to learn all kinds of useful information. For example:
- whether you suffer from any other health problems or chronic diseases
- what pharmaceutical agents you may be taking
- whether you have undergone any surgical procedures and which ones these are
- whether you have any potential mental health problems
- information about potential tobacco and alcohol consumption
- information about potential substance abuse
Then, the physician will take your full sexual history and indicatively will ask you some information, such as:
- description of erectile problem (how rigid erection is and how long it lasts)
- whether there are other sexual problems (low sexual desire, premature ejaculation etc)
- how long ago the problem started
- whether the problem is permanent,periodical or steadily aggravating with time
- whether the sexual partner has any sexual problems (e.g. low sexual desire or reduced vaginal lubrication due to menopause)
- whether erection is successful during masturbation
- whether there are nocturnal and/or morning erections
- whether there are any specific factors aggravating the problem (e.g. place, specific sexual partner etc)
- whether any other therapy has been tried in the past (e.g. erection pills)
Based on the history, the physician can usually evaluate whether the problem is of psychological or organic etiology. Healthy men below the age of 40 who receive no pharmaceutical agents at all and to whom the problem has suddenly occurred, DO NOT need to undergo any diagnostic test! It is obvious that the problem is purely psychological and the Urologist will refer them straight to the Trained Sexologist.
Which are the ED diagnostic tests?
For most patients, a good history (medical and sexual) and clinical examination are enough to set the diagnosis. However, should your physician consider it necessary, you will be asked to undergo some more specific tests, such as:
- Blood tests (blood sugar, cholesterol, testosterone etc). In case the blood test results indicate high risk for coronary disease, you may be referred for cardiological evaluation.
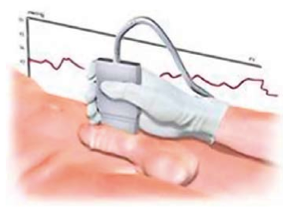
- Triplex Ultrasound of penile vasculature. The physician induces erection (usually by injecting a drug that stimulates erection) and with the use of a special ultrasound device evaluates the penile blood flow and condition of vessels (arteries and veins). This test lasts about one hour.
- Nocturnal Penile Tumescence (NPT). This test aims at recording the number and quality of nocturnal erections with the use of a special device that is attached to the penis before sleep. NPT is conducted at home and helps the physician differentiate between psychogenic and organic erectile dysfunction.
- If there are indications for a psychological problem, the Urologist will refer you to a Trained Sexologist or Psychiatrist accordingly.
Is there a test discriminating between psychogenic and organic ED??
 From birth until the moment an organic erectile problem occurs, every man has 2-6 episodes of erections during an 8-hour sleep. Only if he happens to wake up during the erection, will he become conscious of it. It is possible to record these nocturnal erections with the use of a device called Rigiscan™. The man takes the portable device at home and activates it for 2-3 nights. Then he returns the device to the Urologist and results will be analyzed by the computer. If the test demonstrates high-quality nocturnal erections, the problem seems to be of psychological origin. If there are no good nocturnal erections, then he should undergo a Triplex Ultrasound of the penis.
From birth until the moment an organic erectile problem occurs, every man has 2-6 episodes of erections during an 8-hour sleep. Only if he happens to wake up during the erection, will he become conscious of it. It is possible to record these nocturnal erections with the use of a device called Rigiscan™. The man takes the portable device at home and activates it for 2-3 nights. Then he returns the device to the Urologist and results will be analyzed by the computer. If the test demonstrates high-quality nocturnal erections, the problem seems to be of psychological origin. If there are no good nocturnal erections, then he should undergo a Triplex Ultrasound of the penis.
How is Vascular Erectile Dysfunction diagnosed (VED)?
 If you are above 50 years old with cardiovascular risk factors (high cholesterol or triglycerides, hypertension, diabetes mellitus) or suffer from cardiovascular disease, then you may need to undergo a specific diagnostic test called Ultrasound Triplex of penile vasculature. This test lasts about 1 hour and is done at the physician's office. The physician induces erection (by injecting a drug that stimulates erection) and with the use of a special ultrasound device evaluates penile blood flow. The test results are useful and reliable ony when the physician manages with the drug injection to help you achieve an erection proportional to your best erection achieved at home or during sexual intercourse.
If you are above 50 years old with cardiovascular risk factors (high cholesterol or triglycerides, hypertension, diabetes mellitus) or suffer from cardiovascular disease, then you may need to undergo a specific diagnostic test called Ultrasound Triplex of penile vasculature. This test lasts about 1 hour and is done at the physician's office. The physician induces erection (by injecting a drug that stimulates erection) and with the use of a special ultrasound device evaluates penile blood flow. The test results are useful and reliable ony when the physician manages with the drug injection to help you achieve an erection proportional to your best erection achieved at home or during sexual intercourse.
What therapeutic options are available today?
The type of erectile dysfunction determines the therapy.
Should the etiology be psychogenic factors or relationship problems,a Trained Sexologist can help you overcome the problem. Often, when the problem is of mixed type, a combination of psychotherapy and pharmacotherapy is recommended.
For ED of organic etiology, the therapeutic options available today are the following:
- Oral drugs. Today there are four different pharmaceutical agents: avanafil, sildenafil, vardenafil and tadalafil. Your therapist physician will give you detailed instructions on their administration for achieving optimal efficacy.
- Erectile Dysfunction Shock-Wave Therapy (EDSWT). It is a novel and probably the only therapy available today, which aims at the actual cause of vascular erectile dysfunction.
- Vacuum Pump Device. A special device is inserted into the penis creating air vacuum and inducing blood inflow and penile tumescence. Then a ring is placed around the base of the penis to maintain erection. It is important to know that the ring should not remain there for longer than 30 minutes. This therapy is well tolerated by younger patients, since it does not induce rigid erection.
- Intracavernous Injection Therapy. Your doctor will educate you how to do an injection to your penis whenever you want to achieve erection. This procedure is easy to learn and applied in million patients all over the world. It is important to determine the proper dose, so as to avoid the major injection complication called 'priapism' (=persistent painful presence of erection unrelated to sexual stimulation. This complication requires immediate medical treatment)
- Hormonal therapy. It is applied in a small number of patients with testosterone deficiency. The physician prescribes the appropriate medicinal preparations so that testosterone resumes to normal levels. Today there is an injectable formulation used (one injection every 3 months), as well as topical skin therapies in spray or gel form.
- Penile Prosthesis. It is applied when all other previously mentioned therapies have failed. A special device is surgically placed into the penile cavernous bodies, for inducing erection when the patient wants to. High cost is one of the main disadvantages of the method. Complications, though rare, are contamination and rejection of the prosthesis (5% of cases). Patients have to be well informed before procceeding to a penile prosthesis, in order to avoid false expectations.
Your therapist physician will recommend the therapy or combination of therapies that is mostly appropriate for your individual case.
What are the most widely applied ED therapies today?
Should ED be of psychological origin, there are special therapies (Cognitive/ Behavioral and Sex therapy), including one session about every 2 weeks with a Trained Sexologist for a period of 1-3 months depending on the problem.
When the problem is of organic etiology, the most common treatment is pharmacotherapy. It has to be pointed out that erection pills are used by men with psychogenic erectile dysfunction, until the problem is ultimately resolved.
How effective and safe are erection pills?
It was in 1998 when Viagra™ (sildenafil) was first introduced into the market. Five years later, followed Cialis™ (dadalafil) and Levitra™ (vardenafil), while in 2013 came Spedra™ (avanafil). Since then, more than 200 million men have used the above worldwide. For, they are extremely effective in 50-70% of cases, according to the severity of the problem. In addition, the 17-year experience has clearly demonstrated that all 4 drugs are equally safe. The only absolute contraindication is co-administration with nitrates (medication to treat angina).
Do erection drugs differ one from another?
They are all effective and safe. They are used 1-2 hours before sexual intercourse, while avanafil can also be taken 30 minutes after food intake. There are two differences: a) avanafil, tadalafil and the new forms of mouth-dissolving sildenafil and vardenafil are not affected by food intake, and b) tadalafil action lasts 36 hours, whereas the other two preparations last 4-12 hours, according to the severity of erectile dysfunction. It should be noted that tadalafil is also available in daily small 5mg doses, indicated for those who have frequent sexual contact. This form has been approved since three years ago to be also given to patient with urinary problems due to prostate hypertrophy, given that erection drugs have been proven to significantly improve urination.
How many Greek men take oral ED drugs today?
According to official drugstore sales data (and not according to internet information), about 400.000 pills are sold every month. There are many packages available but the most commonly used is the package of 4 tablets. It is estimated that more than 100.000 Greek men use one of the different erection pharmaceutical agents.
If erection pills are not effective, what other therapeutic options are available?
Should erection pills not be effective, there are intra-penile injections available. A special drug is infused into the penis with the use of a fine needle (like the one used for insulin injection). This method has been used since 1985. Its action starts within 10 minutes from the moment of injection with a duration that, depending on the dose, should not exceed 1 hour. It is a well-tested therapy with very few complications as long as the appropriate dose has been prescribed by an experienced Urologist.
Besides pharmacotherapy, what other therapeutic options are available?
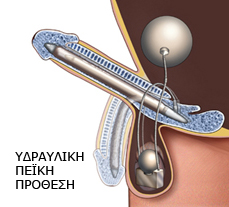 In case pharmacotherapy fails, there is the option of penile prosthesis. Penile prostheses are so much technologically advanced today that they are guaranteed for a lifetime. They are placed surgically into the scrotum with a suture that is not visible postoperatively. The patient can activate the prosthesis whenever and for any duration it is desired. It should be underlined that penile prostheses are an excellent therapy for patients who have undergone oncological pelvic interventions (e.g. radical prostatectomy and colectomy) and therefore there is damage of peripheral nerves controlling erection. Also, it is indicated for patients with traumatic injuries of the spinal cord or pelvis.
In case pharmacotherapy fails, there is the option of penile prosthesis. Penile prostheses are so much technologically advanced today that they are guaranteed for a lifetime. They are placed surgically into the scrotum with a suture that is not visible postoperatively. The patient can activate the prosthesis whenever and for any duration it is desired. It should be underlined that penile prostheses are an excellent therapy for patients who have undergone oncological pelvic interventions (e.g. radical prostatectomy and colectomy) and therefore there is damage of peripheral nerves controlling erection. Also, it is indicated for patients with traumatic injuries of the spinal cord or pelvis.
What is the new method of Erectile Dysfunction Shock-Wave Therapy (EDSWT)?
Until today, therapies for erectile dysfunction of vascular etiology would occasionally treat only the symptom but not the actual cause, that is reduced blood flow in penile cavernous bodies. However, it seems that this novel therapeutic method renders feasible the threatment of the disease itself, for Shock Waves induce penile revascularization.
What are Shock Waves (SW)?
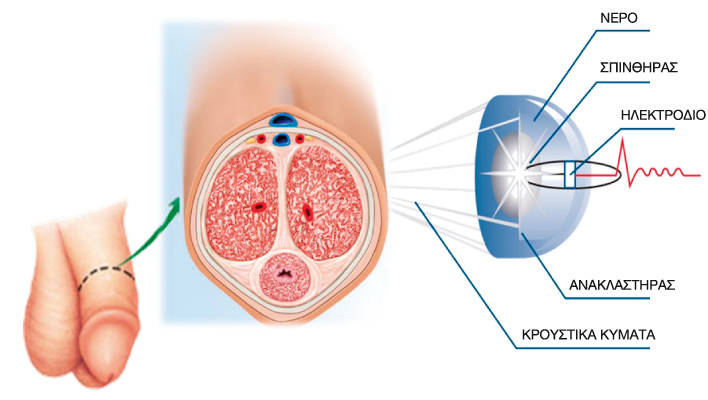 Shock Waves are high-energy electrohydraulic waves (Omnispec™ device), similar to the waves used therapeutically in many medical specialties, such as Urology, Orthopedics, Cardiology and Otorhinolaryngology. In an non-invasive way, the Urologist uses a special probe with mirrors on the penile skin to convey shock waves to the target-site (cavernous bodies of the penis).
Shock Waves are high-energy electrohydraulic waves (Omnispec™ device), similar to the waves used therapeutically in many medical specialties, such as Urology, Orthopedics, Cardiology and Otorhinolaryngology. In an non-invasive way, the Urologist uses a special probe with mirrors on the penile skin to convey shock waves to the target-site (cavernous bodies of the penis).
How is EDSWT applied and how effective is it?
Erectile Dysfunction Shock-Wave Therapy (EDSWT) includes 12 sessions of 30 minutes each for a period of 9 weeks. It is absolutely painless and has no side-effects at all. Cases in which this method was applied demonstrated increase of penile blood flow by 140%, while 80% of patients discontinued erection drug therapy after undergoing EDSWT. According to a recent study, EDSWT is highly effective in cases which do not respond to pharmacotherapy. It has been shown that, after a shock-wave therapy, 70% of men will respond to pharmaceutical drugs for erectile dysfuntion.

How effective are drugs that are advertised on T.V./mass media and are purchased from drugstores without medical prescription? Should we trust them?
No. A drug is tried for about 10 years in various pharmacological and clinical trials and goes through very strict 'tests" before being approved by central regulatory authorities in Europe, America and Greece. However, this does not apply for preparations coming from 'natural/plant extracts', which are allowed to be available in the market without having been tested. You will see them on drugstore shelves in packages with labels stating that they help masculinity or erection and they are even advertisted on T.V. despite the lack of relevant studies.
How safe are drugs ordered online (on the Internet)?
We do not know what they contain or whether the composition written on the package is true. Studies have shown that very often they DO NOT contain the ingredients that are written on the package and, thus, are dangerous. Ordering drugs from online pharmacies (via Internet) is highly dangerous because the packages may be the same as those of officially approved drugs but the content may be completely different. That is the reason why the European Union has adopted a Special Directive related to the risk of purchasing falsified medicinal products from the internet.
Do also men without ED take erection drugs?
There is no doubt that some men use them just for reasons of 'lifestyle', that is purely for 'showing off their performances'. In fact, they actually help the penis to increase its blood perfusion. However, this 'lifestyle use' is surely an 'abuse' and is actually done to cover a man's insecurity and lack of self-confidence. It is always harmful for our body to take drugs for no real reason and without medical prescription.
What can I do for Prevention?
To read about prevention of erectile dysfunction, click here.