
Though flexible at rest (relaxation), the penis becomes hard and straight with sexual arousal, for it fills up with blood. Both these features are essential for carrying out its function during sexual intercourse.
But, is the erect penis always and in all men straight? In the majority of men it is;even though there may be slight deviations of 10-15 degrees in most men, this is not a problem.
However, some men are born with congenital penile curvature, a disease in which the penis presents a curvature, usually downwards. The most common cause is the uneven growth of the membrane surrounding the penis (tunica albuginea). In more rare cases penile curvature may be due to abnormal anatomy of the urethra which is shorter than the penis and therefore keeps it bent downwards.
These curvatures may be mild (up to 30 degrees) and not bother the penile function or prevent vaginal penetration. Of course, some curvatures, even though not preventing penile function, affect young men psychologically purely from an aesthetic point of view.
There are other cases in which men may see their penis bending and changing direction at some point of their life. The first reaction is fear, particularly in cases when erection is accompanied with pain. However, unfortunately only very few of them will immediately consult the trained Urologist, because they hope that this bending is temporary. But this is not true, for the pain may be gone with time but not the curvature which will remain and, in some cases, may even increase.
This is called Peyronie's Disease. It may occur randomly in 3-9% of men (according to age) and is not related with infections or cancer. Nobody has ever died of the disease, but many have lost their sexual life because of it.
The most common etiology is a small penile injury during sexual intercourse. Particularly in men with cardiovascular risk factors (diabetes mellitus, hypertension, high cholesterol etc), natural healing of the injury is not possible and the wound becomes a hard scar making the outer membrane shrink; thus, the penis loses length from one side and bends towards the side of the scar.
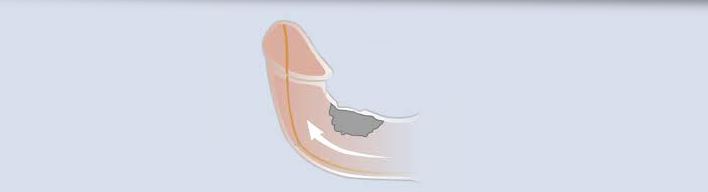
Fracture
In rare cases, tunica albuginea may be ruptured extensively during sexual intercourse; this usually happens in a specific sexual position, when the female partner presses and squeezes the penis with her body weight, causing the so-called 'penile fracture'.
This is a very painful experience, since it is accompanied with excruciating pain and massive penile hematoma. The penile fracture is an emergency surgical disease, since its delayed treatment (beyond 6-8 hours) may be followed with permanent erectile dysfunction.
Peyronie's disease is characterized by hard plaques (scar tissue lumps) on the shaft of the penis. The formation of these plaques causes penile bending and angling during erection. In some cases, this bending may be so extensive that the penis cannot penetrate and, as a result, sexual intercourse is not possible.
This condition dates back to the 6th century B.C. but took its name after F. G. de la Peyronie, who in 1743 described the characteristic fibrotic and sometimes calcified plaques underneath the penile skin.
Peyronie's disease may afflict any man. It most frequently occurs at the age of 50 but this does not exclude the possibility of occurring also in men of young age.
The disease is not so rare as it is believed. It is roughly estimated that the number of men suffering in Greece amount to 20.000. The actual number is probably bigger, as many are the men who unfortunately refuse to visit the medical expert when the first symptoms of penile pain or angling occur, simply because they fear they may suffer from something worse.
Consequences
The three main symptoms of the disease are local pain, palpable hard lumps on the shaft of the penis and penile bending, usually upwards, or rotation rightwards or leftwards.
Symptoms differ in severity and are not observed in all patients.
At first, some men experience penile pain during erection, which often subsides without treatment.
As plaques increase in size, the erect penis starts showing some curvature or angling, which ends up in penile deformity that most of the times makes sexual intercourse exceptionally difficult or impossible or highly distressful for both partners.
From an aesthetic point of view, it significantly affects male psychology, particularly at younger ages or in men with a stable long-term relationship.
However, it is inevitable that sometimes sexual intercourse problems will cause tension on both sides even in a long-term relationship. The psychological burdening that is estimated in 80% of the men with the disease may be disruptive, no matter how understanding the female partner may be.
Sometimes the anxiety caused and difficulties arising during sexual intercourse may lead to psychogenic erectile dysfunction. In 20% of the cases, once the hard plaque expands and includes penile arteries, the blood flow is interrupted and erection is no longer possible.
Therapeutic treatment
The treatment of the disease is imperative when the penile curvature is such that prohibits the vaginal penetration during sexual intercourse. At first stage (before the plaque gets permanent), the treatment is pharmaceutical, but when the plaque gets consolidated (usually within one year), only surgery is indicated.
Medications
Although many pharmaceutical agents have been used for the conservative treatment of Peyronie's disease, very few studies have shown moderate efficacy and, of course, none of them is effective in all cases.
Medications administered with limited efficacy are tamoxifen, colchicine and vitamin E. As for others, such as para-aminobenzoic acid (PABA), there are no results available coming from comparative placebo-controlled studies.
In addition, other agents have been tried, injected directly into the scar on the penis, such as verapamil when the penile bend does not exceed 30 degrees, also with moderate or poor results though.
Surgical procedures
Surgery is indicated when the penile curvature is over 60 degrees. However, if the bend is relatively small (40-60 degrees, usually at young age) but the patient's psychology is negatively affected, then surgery is also recommended. It is absolutely indicated when the penile deformity is such that causes difficulty in sexual intercourse. This happens in about 20-30% of cases.
It is essential that the injury stabilizes before surgical intervention. Therefore, the first diagnostic steps are medical history, physical examination and ultrasound scan of the penis that provides a lot of information about the size and composition of the plaque. Otherwise, the disease will relapse despite the initial straightening of the penis, as fibrosis progresses and the plaque expands.
Many types of surgical interventions and techniques have been described. Corporeal plication with partial excision of tunica albuginea is widely applied in Peyronie's disease. It gives excellent long lasting results, with relapse rate below 10% in congenital curvatures and below 20% in Peyronie's disease.
The surgical operation includes excision of a tissue block from the contralateral (normal) side , i.e. from the covnex side of the penis, in order to straighten the penis.
This plication can be conducted without the partial removal of the penile fibrous tissue. However, the main disadvantage of plication is the reduction of penile length by about 1-1/2 cm. Taking into account that the average penile length in erection is 12,8-14,5cm, according to published studies, the length reduction is not a problem in men with length below 13 cm.
It is likely to have relapse (recurrence) of the curvature and this is mainly due to the progression of the disease or to the rupture of sutures placed on the tunica albuginea. Although today this is considered to be the surgical procedure of choice, the surgeon should know all techniques and always decide which is the most suitable for each individual case.
The use of grafts (of biological or synthetic materials) constitutes another therapeutic method, followed by less postoperative length reduction of the penis but with higher rate of postoperative erectile dysfunction.
Removal of the fibrous plaque is avoided, for it often leads to erectile disorders due to insufficient blood supply in the graft area. In these cases, penile prosthesis implantation is a highly reliable method -despite the high cost of the prostesis- in men with vascular lesions, erectile dysfunction and penile curvature.
What should patients do
The moment you feel pain or palpate any lump on the penis, go straight to your doctor. If you are diagnosed with Peyronie's disease, ask your doctor to inform you in detail about this condition and the available therapeutic options.
Do not just sit at home and forget it. If your doctor is not in the position to answer your questions with regard to your problem and does not provide you sufficient advice, it is better to address to a Trained Urologist specialized in andrological issues.
There are organised medical offices and clinics in various cities dealing with male sexual problems.
Sometimes the disease may subside spontaneously (10-20% of cases), but you should be under medical supervision. You should remember that there are available treatments and that the sooner your problem is treated, the greater and more substantial help you will receive.
Your partner's support and understanding is of high significance. If you learn as much information as possible about the disease and share this information with your partner, then already a great part of your anxiety and stress will be released.